
Individual-level Strategies
Overall Goal: Develop and Implement a Campus-wide System to Screen, Identify, and Intervene with Students who are at Risk for Alcohol-related Problems
 One of the most critical components of a campus strategic plan to address college student drinking is the design and implementation of a system by which college students who are at varying levels of risk get the appropriate level of services. Research tells us that college students who need services rarely get them.3 This is due in part to the low self-recognition of problems among students, as well as the lack of campus resources to screen students and to provide services.
One of the most critical components of a campus strategic plan to address college student drinking is the design and implementation of a system by which college students who are at varying levels of risk get the appropriate level of services. Research tells us that college students who need services rarely get them.3 This is due in part to the low self-recognition of problems among students, as well as the lack of campus resources to screen students and to provide services.
The first part of such a system is understanding the population of students with respect to their drinking patterns. A campus needs to be proactive and systematic about identifying at-risk students by screening in many different settings. The second part of the system is a plan to route students with different drinking patterns toward an appropriate level of intervention and monitor their outcomes. How frequently a student with an alcohol problem receives such interventions should be ideally tailored to the level of severity of their problem, but it is understood that there are constraints on resources that might make the ideal scenario unrealistic. Colleges should, at the very least, form relationships with providers in the community that can offer more intensive services to students with the highest level of problems. Referrals can then be made to these providers.
Overview
The first part of this section describes the various approaches that can be used to change individuals’ drinking behavior, followed by educational approaches that can be used to increase knowledge about risks.
It is important to note the difference between the goals of interventions and education. While education can increase knowledge or raise awareness, research has shown that it is not effective in changing individual behavior. Behavior change is a much more difficult challenge and requires more intensive efforts like motivational interviewing (MI) and cognitive behavioral therapy (CBT).
INVISIBLE - DO NOT DELETE
Overview ... continued
In the next part of this section, the various settings and contexts in which students can be identified and screened for high-risk drinking behavior are described. There are multiple settings in which students can be identified. Because many students will enter college with high-risk drinking patterns that began during high school, screening of first-year students is necessary to identify the students at highest risk for alcohol problems. However, because high-risk drinking can occur throughout young adulthood, opportunities for screening and interventions for students in all stages of their college career should be provided.
Students might also be identified as potentially high-risk drinkers because they violated a campus alcohol policy. For these students, strategies should be in place to identify the severity of their drinking problem before deciding on a course of action for the student. Evaluating their risk for recidivism is an important component in deciding the frequency of monitoring that might be necessary. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) has useful guidelines for clinicians that can be found here.
Primary health care settings offer two more opportunities for screening and intervention. Students seeking routine care can be screened for high-risk drinking as well as students who present with a problem that is more directly related to excessive drinking (e.g., alcohol-related injuries). Because of the known relationship between excessive drinking and academic performance,18,19 students who are mandated to receive services from the academic assistance center or who voluntarily seek services are also candidates for screening.
Athletic programs, fraternities, and sororities offer yet additional opportunities to screen and identify students with alcohol problems. It is fully recognized that each college will vary significantly with respect to the number and types of settings in which students can be realistically identified. For example, many schools do not have a Greek system, and many two-year schools do not have health centers, so therefore the material on these settings might not be applicable to them.
This Guide also describes how faculty, resident advisors, and students can be made aware of their role in the “routing process”—that is, to simply identify, approach, and facilitate referrals to appropriate places on campus for further screening and evaluation. These individuals can be empowered and supported in an ongoing way to play this important role.
Schools vary significantly with respect to their ability to triage high-risk cases to appropriate levels of services. Ideally, a college should try to identify not only students who are exhibiting obvious signs of risky behaviors, but also those who might be at risk for developing alcohol problems. Moreover, individual-based strategies might have limited success if the individual is placed back into the same high-risk environment from which they came. Therefore, more general population-based strategies are also needed to address campus alcohol problems.
Another common finding is that short-term gains do not necessarily translate into long-term changes in behavior, unless the intervention is sustained. This can be frustrating to clinical professionals, but it makes sense if one realizes that excessive drinking is a well-established habit for many students, one that is difficult to change. Just like weight loss involves a change in the way a person identifies with food and requires ongoing vigilance, reductions in drinking behavior will require intensive and long-term monitoring.
These kinds of long-term continuous strategies to monitor alcohol use might be cost-prohibitive for schools to implement, especially if they involve regular meetings with a highly trained professional. Although long-term research studies have not been conducted among college students to determine the effectiveness of recording one’s drinking with a drinking diary or calendar, these low-cost methods have shown promise in other populations and therefore should be considered as potential strategies to reduce excessive drinking.
Research-based interventions that are designed to reduce individual behavior cannot be seen as a magic bullet, especially given the modest, albeit statistically significant, reductions that have been observed in research studies. Individually-targeted interventions by themselves are unlikely to lead to the kind of sustained changes at the population level that most colleges and communities would define as success. They need to be coupled with effective environmental strategies for multilevel, multi-component interventions.
Step 1. Choose a Screening Instrument
To estimate the level of alcohol consumed, standard assessments inquire about both quantity (the amount of alcohol) and frequency (how often one drinks alcohol). An example of a question that assesses quantity is “How many drinks do you consume during a typical weekend day?” An example of a question that assesses frequency is “How many days during the past month did you drink alcohol?” It is preferable to ask questions about how much or how often someone drinks rather than a simple yes or no question such as “Do you drink alcohol?” With yes or no questions, the person might choose to avoid any follow-up conversation by simply saying no. Questions that assume a person drinks, such as the quantity and frequency questions mentioned above, can therefore enhance honesty. Non-drinkers can simply say “I don’t drink” or “None.” A third dimension of screening focuses on the consequences that one has experienced as a result of their drinking. It is preferable to not label these consequences as “problems,” since many students will not necessarily recognize consequences as problems. The federally-sponsored National Survey on Drug Use and Health20 contains questions that measure alcohol abuse and dependence according to standard psychiatric criteria.21
There are a number of scientifically-validated screening instruments that can be easily used in college settings.22 Winters et al.22 found that the CAGE questionnaire23 was most frequently used for college settings. Other commonly used instruments among the college population are the AUDIT7 and the CRAFFT.24 Cook et al.25 found that the AUDIT, which contains ten items, was more effective than the CAGE and the CRAFFT in detecting alcohol use disorder among young adults. DeMartini and Carey26 found that the shortened form of the AUDIT that contains three items, the AUDIT-C, performed even better than the AUDIT in detecting alcohol use disorder among college students.
It is important for schools to decide on the purposes of screening before choosing a screening tool. Is the screening tool simply used to identify students who need more comprehensive assessment? In that case, it might be necessary to have a brief screening tool that separates current drinkers from non-drinkers. Although it is understandable that schools would prefer to use a screening instrument with the fewest number of items, obtaining comprehensive information about the student’s problem is a critical first step in understanding how best to intervene. Therefore, the value of a longer screening instrument should not be discounted if it will help achieve the goals of screening. Also, screening tools can be made widely available online for self-assessments or for peers to assess a potential problem in a friend.
Step 2: Implement a System to Screen and Identify Students
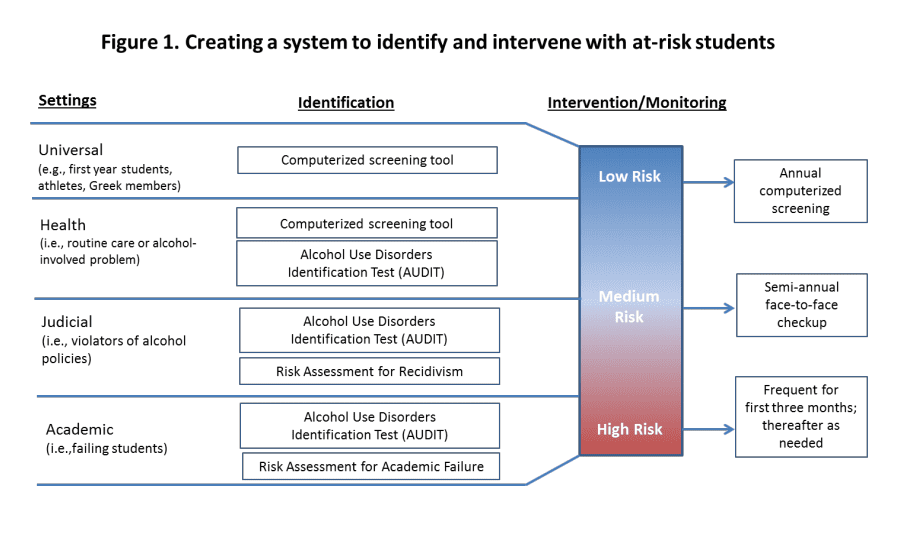
As mentioned earlier in the section on developing a strategic plan, it is important for campuses to design a “roadmap” to identify, screen, and refer students for appropriate levels of care that is tailored to their campus’s resources and needs. Figure 1 is a comprehensive example of a roadmap, with hypothetical suggestions for how often different types of students would be monitored for follow-up. This Guide describes a number of settings in which screenings can be implemented.
Step 3: Develop Criteria for Directing Students to Appropriate Resources
As can be seen in the model displayed in Figure 1, students are classified into three categories (low, medium, and high risk) based on the results of their screening. Although the screening instruments themselves provide such guidelines, the number of students falling into a high-risk category might overwhelm the resources for a particular campus, and thus schools will need to decide what those cut-points are and how students with different levels of need are routed to different levels of interventions or given referrals to additional resources.
 Step 4: Monitor Student Progress
Step 4: Monitor Student Progress
 Step 4: Monitor Student Progress
Step 4: Monitor Student ProgressIdeally, schools should monitor two features of this system. First, it is necessary to monitor the implementation of the system. For example, it is important to know what proportion of students coming through the health center were screened, and what proportion of students who screened positive were given a more extensive assessment and/or referred for an intervention. Studies have shown that performance measurement systems can be very helpful in increasing the effectiveness of interventions over time. It might not be realistic, especially if the system is new, to expect that every student will be tracked through all settings and monitored for progress, but designing a plan for measuring even a subset of students and slowly expanding it over time is essential. Second, monitoring of individual student progress can be accomplished through a variety of mechanisms using technology as appropriate.
Step 1. Choose a Screening Instrument
To estimate the level of alcohol consumed, standard assessments inquire about both quantity (the amount of alcohol) and frequency (how often one drinks alcohol). An example of a question that assesses quantity is “How many drinks do you consume during a typical weekend day?” An example of a question that assesses frequency is “How many days during the past month did you drink alcohol?” It is preferable to ask questions about how much or how often someone drinks rather than a simple yes or no question such as “Do you drink alcohol?” With yes or no questions, the person might choose to avoid any follow-up conversation by simply saying no. Questions that assume a person drinks, such as the quantity and frequency questions mentioned above, can therefore enhance honesty. Non-drinkers can simply say “I don’t drink” or “None.” A third dimension of screening focuses on the consequences that one has experienced as a result of their drinking. It is preferable to not label these consequences as “problems,” since many students will not necessarily recognize consequences as problems. The federally-sponsored National Survey on Drug Use and Health20 contains questions that measure alcohol abuse and dependence according to standard psychiatric criteria.21
There are a number of scientifically-validated screening instruments that can be easily used in college settings.22 Winters et al.22 found that the CAGE questionnaire23 was most frequently used for college settings. Other commonly used instruments among the college population are the AUDIT7 and the CRAFFT.24 Cook et al.25 found that the AUDIT, which contains ten items, was more effective than the CAGE and the CRAFFT in detecting alcohol use disorder among young adults. DeMartini and Carey26 found that the shortened form of the AUDIT that contains three items, the AUDIT-C, performed even better than the AUDIT in detecting alcohol use disorder among college students.
It is important for schools to decide on the purposes of screening before choosing a screening tool. Is the screening tool simply used to identify students who need more comprehensive assessment? In that case, it might be necessary to have a brief screening tool that separates current drinkers from non-drinkers. Although it is understandable that schools would prefer to use a screening instrument with the fewest number of items, obtaining comprehensive information about the student’s problem is a critical first step in understanding how best to intervene. Therefore, the value of a longer screening instrument should not be discounted if it will help achieve the goals of screening. Also, screening tools can be made widely available online for self-assessments or for peers to assess a potential problem in a friend.
Step 2: Implement a System to Screen and Identify Students
As mentioned earlier in the section on developing a strategic plan, it is important for campuses to design a “roadmap” to identify, screen, and refer students for appropriate levels of care that is tailored to their campus’s resources and needs. Figure 1 is a comprehensive example of a roadmap, with hypothetical suggestions for how often different types of students would be monitored for follow-up. This Guide describes a number of settings in which screenings can be implemented.
Step 3: Develop Criteria for Directing Students to Appropriate Resources
As can be seen in the model displayed in Figure 1, students are classified into three categories (low, medium, and high risk) based on the results of their screening. Although the screening instruments themselves provide such guidelines, the number of students falling into a high-risk category might overwhelm the resources for a particular campus, and thus schools will need to decide what those cut-points are and how students with different levels of need are routed to different levels of interventions or given referrals to additional resources.
Step 4: Monitor Student Progress
Ideally, schools should monitor two features of this system. First, it is necessary to monitor the implementation of the system. For example, it is important to know what proportion of students coming through the health center were screened, and what proportion of students who screened positive were given a more extensive assessment and/or referred for an intervention. Studies have shown that performance measurement systems can be very helpful in increasing the effectiveness of interventions over time. It might not be realistic, especially if the system is new, to expect that every student will be tracked through all settings and monitored for progress, but designing a plan for measuring even a subset of students and slowly expanding it over time is essential. Second, monitoring of individual student progress can be accomplished through a variety of mechanisms using technology as appropriate.
Step 2: Implement a System to Screen and Identify Students
Step 2: Implement a System to Screen and Identify Students
As mentioned earlier in the section on developing a strategic plan, it is important for campuses to design a “roadmap” to identify, screen, and refer students for appropriate levels of care that is tailored to their campus’s resources and needs. Figure 1 is a comprehensive example of a roadmap, with hypothetical suggestions for how often different types of students would be monitored for follow-up. This Guide describes a number of settings in which screenings can be implemented.
Step 3: Develop Criteria for Directing Students to Appropriate Resources
As can be seen in the model displayed in Figure 1, students are classified into three categories (low, medium, and high risk) based on the results of their screening. Although the screening instruments themselves provide such guidelines, the number of students falling into a high-risk category might overwhelm the resources for a particular campus, and thus schools will need to decide what those cut-points are and how students with different levels of need are routed to different levels of interventions or given referrals to additional resources.
Step 4: Monitor Student Progress
Ideally, schools should monitor two features of this system. First, it is necessary to monitor the implementation of the system. For example, it is important to know what proportion of students coming through the health center were screened, and what proportion of students who screened positive were given a more extensive assessment and/or referred for an intervention. Studies have shown that performance measurement systems can be very helpful in increasing the effectiveness of interventions over time. It might not be realistic, especially if the system is new, to expect that every student will be tracked through all settings and monitored for progress, but designing a plan for measuring even a subset of students and slowly expanding it over time is essential. Second, monitoring of individual student progress can be accomplished through a variety of mechanisms using technology as appropriate.
Step 3: Develop Criteria for Directing Students to Appropriate Resources
As can be seen in the model displayed in Figure 1, students are classified into three categories (low, medium, and high risk) based on the results of their screening. Although the screening instruments themselves provide such guidelines, the number of students falling into a high-risk category might overwhelm the resources for a particular campus, and thus schools will need to decide what those cut-points are and how students with different levels of need are routed to different levels of interventions or given referrals to additional resources.
Step 4: Monitor Student Progress
Ideally, schools should monitor two features of this system. First, it is necessary to monitor the implementation of the system. For example, it is important to know what proportion of students coming through the health center were screened, and what proportion of students who screened positive were given a more extensive assessment and/or referred for an intervention. Studies have shown that performance measurement systems can be very helpful in increasing the effectiveness of interventions over time. It might not be realistic, especially if the system is new, to expect that every student will be tracked through all settings and monitored for progress, but designing a plan for measuring even a subset of students and slowly expanding it over time is essential. Second, monitoring of individual student progress can be accomplished through a variety of mechanisms using technology as appropriate.
Approaches
INVISIBLE - DO NOT DELETE
Strategy: Utilizing Cognitive Behavioral Therapy
Theory Behind the Strategy
Cognitive behavioral therapy (CBT) is grounded in the idea that thoughts play a central role in behavior. It is a general clinical strategy that teaches skills to modify one’s beliefs. Working with a clinician, a student begins to understand how s/he might be relying too much on assuming things rather than carefully evaluating whether or not something is true. By identifying “automatic thinking errors,” the student can then begin to change the way they are thinking about something and subsequently change their behavior as a result. For example, a student might be thinking that drinking alcohol is necessary to reduce stress or to feel more socially comfortable. By questioning these sorts of assumptions, a student can change his/her drinking behavior.
Evidence of Effectiveness
There is a wealth of scientific evidence supporting the use of CBT for a variety of psychiatric disorders, including substance abuse and dependence. If applied with fidelity in a sufficient number of sessions, CBT is considered to be one of the most effective counseling strategies for changing behavior. In a college setting, however, single sessions might be more feasible than multiple sessions. Samson and Tanner-Smith28 reviewed evidence on various single-session intervention approaches for heavy-drinking college students, including CBT, educational approaches, motivational interviewing, and personalized feedback. Effect sizes for interventions using CBT were not significant, and the authors concluded that findings were inconclusive due to a large standard error, possibly because of variation in how it was implemented in the individual research studies. Thus, CBT appears to be better suited for students with alcohol dependence because of its more intensive multiple-session approach, whereas a single session intervention might be more appropriate for students who are at risk for developing dependence.
Tips for Implementation
As stated previously, students at the highest level of severity of drinking problems are most appropriate for CBT. CBT is best applied in clinical settings with health professionals who have received special training. If resources allow, schools can have a number of staff trained in CBT for the most severe cases, but also have referrals to others in the community who are extensively trained and provide CBT services. Interventions utilizing motivational interviewing, which are described next, can be used for students whose drinking problems are not as severe.
Strategy: Utilize Motivational Interviewing
Theory Behind the Strategy
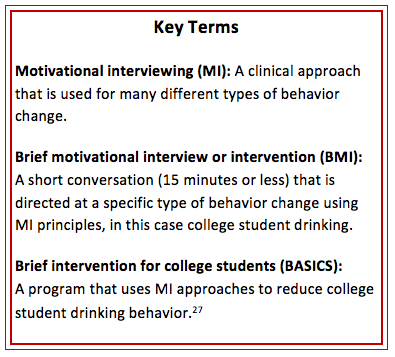
Motivational interviewing (MI) in a college setting can be viewed as a “collaborative conversation” between a student and a health professional. The goal is to identify and capitalize on the student’s ambivalence about their drinking behavior. By listening very carefully to how a student describes his/her drinking behavior, a clinician can reflect the student’s own words to elicit internal motivations to change behavior. Alcohol use is assessed with nonjudgmental feedback, and then the clinician provides suggestions for behavioral options without confrontation.29
MI is based on three core assumptions: 1) the individual is ambivalent about the need to change his or her drinking behavior; 2) risk or harm reduction is more acceptable to the person than abstinence; and 3) students have the motivation and the skills to use drinking reduction strategies.30 Among college students, MI is generally used in the context of a brief motivational intervention (BMI). BMIs can be a one-on-one session between the student and a counselor or a computer program. They generally last for one hour or less. BMIs often assess the student’s drinking patterns to construct a personal drinking profile (e.g., quantity-frequency consumed, peak blood alcohol level, amount of money spent on alcohol, caloric intake), and then engages the student in a normative comparison exercise (e.g., beliefs about peers’ drinking, amount consumed in relation to peers) while using a non-confrontational MI style.
Evidence of Effectiveness
There is a wealth of scientific studies that support MI to change behavior, many of which have been conducted with college students. MI can effectively reduce both alcohol and drug use,31 as well as negative consequences such as blackouts.32 Many factors influence the impact of this intervention, including the number of sessions, the type of training that the interviewer has received, and whether there are continued follow-ups. The aforementioned meta-analysis by Samson and Tanner-Smith28 found that interventions using MI approaches had the most impact on alcohol use behaviors. Multiple studies show that MI appears to be effective when used alone, compared with other interventions like CBT, psychoeducational therapy, or none at all.28,33
Individual skills-based or motivational enhancement interventions might be as effective in changing college students’ drinking behaviors when the interventions are provided by trained peer counselors as when they are provided by professionals, although the professionals might be more knowledgeable and have better skills.34,35
Research has shown that face-to-face interventions are more effective when they include personalized feedback, discussion of risks and problems, normative comparisons, moderation strategies, challenging positive alcohol expectancies, and blood alcohol concentration (BAC) education.36
BMI has been identified as a potential method to cut down drinking among college students.29 A review by Carey et al.36 found that face-to-face interventions were more effective at producing changes that were maintained at long-term follow-ups than computer-delivered interventions for college drinkers. Although computer-delivered interventions were associated with decreases in alcohol quantity and frequency, these decreases were limited to short-term follow-ups and were not maintained in the long-term.
Borsari and Carey29 looked at the effects of a an intervention program based in MI principles (see Strategy: Utilize the BASICS Program) with students who reported binge drinking at least twice during the past 30 days. The intervention provided students with feedback on five components: personal consumption, perceived drinking norms, alcohol-related problems, related harms situations associated with heavy drinking, and alcohol expectancies. At six weeks, the intervention participants exhibited significant reductions in the number of drinks consumed per week, number of times drinking alcohol during the past month, and frequency of binge drinking during the past month compared with the control group.
Tips for Implementation
It is important for professionals who deliver brief interventions to think creatively about how they can optimally “connect” with a student in order to motivate them to change the way s/he views alcohol as a part of their life. MI is an intervention with guiding principles, and the professional has discretion regarding the types of alcohol-related consequences highlighted with any one particular student. The intervention will be enhanced to the degree that the professional can help the student draw connections between his/her behavior and the achievement of a goal with particular salience to that individual. Likewise, clinicians have discretion with respect to the type of guidance they provide regarding setting individual goals for reducing drinking behavior. For instance, a short-term goal might be to increase the number of abstinent days during the coming month and to monitor one’s progress toward that goal with an electronic diary.
MI includes incorporating personalized feedback and decisional balance exercises. The research evidence related to these components is described below.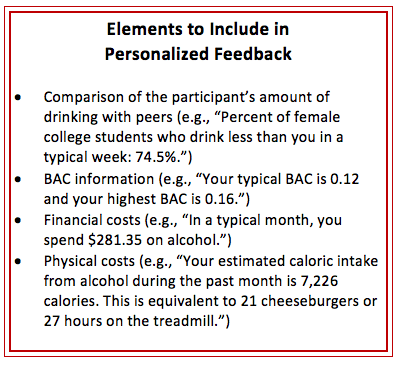
Incorporation of Personalized Feedback
Personalized feedback can be generated based on a discussion during an in-person intervention. This feedback can then be reviewed with the counselor or given to the student to take home. Alternatively, students can complete a screening program on the computer, which then provides a personalized feedback for the student to review. A counselor or physician can then meet with the student to review the personalized feedback, often using the principles of MI.
Evidence of Effectiveness
Doumas et al.37 found that counselor-guided personalized feedback was more effective than self-reviewed personalized feedback at decreasing the mean number of drinks per week and binge drinking episodes during the past two weeks. For example, mandated students who completed a counselor-guided web-based feedback intervention reduced their weekly drinking quantity by about 17% at follow-up, or an average of two drinks per week. Students who completed a self-guided
web-based intervention increased use by about 34%, or three drinks per week. A subsequent study by Doumas et al.38 found that first-year college students who completed a web-based personalized feedback program had fewer sanctions for campus alcohol policy violations compared with an assessment-only control group.
Face-to-face personalized feedback significantly reduced weekly drinking quantity and peak blood alcohol concentration in an intervention among high-risk drinking college students.39 In that study, a computer-delivered personalized feedback intervention with a video interviewer was not associated with significant reductions in drinking. Another study of incoming freshmen found that a computer-delivered personalized feedback-only program was more effective at reducing alcohol use than personalized feedback that included descriptive social norms, although both programs were effective overall.40
Using Decisional Balance Exercises
Decisional balance exercises can be done with or without the assistance of a counselor. Students are asked to write down the pros and cons of changing and not changing their drinking behavior and evaluate their motivation to change.41
Evidence of Effectiveness
Carey et al.36 found that decisional balance exercises were not effective components of either face-to-face or computer-delivered interventions targeted at college students. Specifically, face-to-face interventions that included decisional balance exercises were less effective at reducing quantity of alcohol use than interventions that did not include an exercise, though authors caution that this finding was based on few studies and future research is needed to determine if the approach is ineffective. Participants who received computer-based interventions using decisional balance exercises were less likely to reduce the amount of alcohol consumed both per week/month and per drinking day. Collins et al.42 examined students engaged in decisional balance exercises around current drinking and movement towards reducing drinking. Intervention participants included at-risk students (engaged in weekly, heavy episodic drinking) who participated in a decisional balance worksheet, brief intervention, and various assessment conditions. Decisional balance proportion (which reflected movement toward change) scores reflected greater movement towards change, which in turn best predicted reductions in heavy drinking quantity and frequency as well as alcohol-related consequences.42 While these effects decayed by the 12-month follow-up, the study suggests that decisional balance proportions are a possible measure of motivation to reduce drinking and related harms. A related qualitative study found that a worksheet with an open-ended decisional balance exercise might be better suited for college students than worksheets using Likert-scale questions because it is more personalized and a more accurate representation of what college students actually find to be beneficial or not in changing their drinking habits.43
Strategy: Utilize the BASICS Program
Theory Behind the Strategy
The Brief Alcohol Screening and Intervention for College Students (BASICS) program follows a harm reduction approach using MI techniques. BASICS aims to motivate students to reduce alcohol use in order to decrease the negative consequences of drinking.
BASICS is a program that is conducted during a period of two 50- to 60-minute sessions.27 These sessions include an assessment (or self-report survey) in which the student provides information about his/her current and past alcohol use and attitudes toward alcohol. This assessment information is used to provide personalized feedback around ways to minimize future risk and options for behavior change. The personalized feedback often includes clarifying perceived risks and benefits of alcohol use and comparisons of personal alcohol use to campus- and gender-specific norms. A web program based on BASICS, MyStudentBody.com, has also been developed.
Evidence of Effectiveness
Several studies have shown that high-risk drinkers participating in BASICS reduce the amount they drink significantly both in the short and intermediate term following intervention.29,44,45 A study by Borsari and Carey29 found that compared with the control group, students receiving BASICS drank fewer drinks per week, drank less frequently during the past month, and reduced the frequency of binge drinking during the past month. The number of drinks per week decreased from 17.6 at baseline to 11.4 at follow-up for the intervention group, at the same time that it fell from 18.6 to 15.8 for students in the control group. Drinking occasions per month decreased from 4.4 to 3.8 while the controls remained stable (4.5 to 4.6). Heavy episodic drinking occasions per month decreased for the intervention group from 3.2 to 2.6 and for the controls, from 3.5 to 3.4. A meta-analysis by Carey et al.46 found that BASICS was effective in reducing alcohol-related risks in the short term among mandated students who violated alcohol policies. Terlecki et al.47 conducted the first randomized trial to determine whether the BASICS program was as effective at one year post-intervention for heavy-drinking undergraduates who were mandated to complete the intervention versus heavy-drinking undergraduates who volunteered to participate. They found that the students receiving the BASICS intervention—regardless of whether they were mandated or volunteered–showed significantly fewer alcohol-related problems one-year post-intervention compared with an assessment-only control group.
Strategy: Utilize eCHUG (eCHECKUP TO GO)
Theory Behind the Strategy
The eCHECKUP TO GO program (informally known as eCHUG) is a personalized, online prevention intervention that has separate curricula to address alcohol and marijuana use as well as other health behaviors. Based on MI and social norms theory, this program is designed to motivate individuals to reduce their use using personalized information about their own substance use and risk factors associated with use. eCHUG is individually tailored to each campus and can be shared school-wide among departments.
eCHUG is self-guided and takes about 20 to 30 minutes to complete. Students can complete a personal check-up on multiple occasions to track changes about their use and risk behaviors. If a counselor wishes to use the program in conjunction with face-to-face contact, the student can be asked to complete the companion Personal Reflections program. This feature requires an additional 15 to 20 minutes and asks students to respond to questions designed to further examine their personal choices and the social norms surrounding and influencing their use of substances.
Evidence of Effectiveness
Two research studies compared alcohol outcomes between first-year students receiving eCHUG and an assessment-only control group. Both of these studies showed a significant reduction in the mean number of drinks per week for students who received eCHUG. One study48 found a reduction of 1.43 (with an increase of 6.33 for the control group) at one month post-intervention. The other study, by Doumas et al.,49 observed a decrease in mean number of drinks per week of 0.6 at three months post-intervention, as compared with an increase of 0.3 for the control.
Another study tested the effectiveness of eCHUG among first-year students when added to existing alcohol education programs (Alcohol 101 and CHOICES).50 The four intervention groups included: 1) Alcohol 101 + eCHUG, 2) Alcohol 101 alone, 3) CHOICES + eCHUG, and 4) CHOICES alone. Those in the combined eCHUG conditions reported consuming fewer drinks per hour (an average of 0.4 drinks) compared with curriculum conditions without eCHUG (an average of 1.3 drinks) at a four-week follow-up. This study did not have a control group, so researchers were not able to conclude that eCHUG is effective as a stand-alone intervention for this population; rather, beneficial effects might result when it is used in combination with other education programs.
eCHUG has been found to be more effective among heavier drinkers than lighter drinkers, according to a study that compared eCHUG with a control condition among first-year students.51 Among mandated students, another study found that eCHUG did not significantly decrease alcohol use when compared with BASICS and CHOICES, but it did significantly decrease alcohol-related harms.52
One study compared the drinking behavior of mandated students who received eCHUG with either self-guided feedback versus counselor-delivered feedback.53 Students who received eCHUG with self-guided feedback reduced their drinking by about one drink per week. In comparison, students who received counselor-guided feedback saw a decrease of about four drinks per week, suggesting that eCHUG might work best when in conjunction with other treatment and prevention methods.
Strategy: Challenge Alcohol Expectancies
Theory Behind the Strategy
Many college students are under the impression that alcohol use carries with it a number of social benefits, including an increased sense of well-being and relaxation, being more socially comfortable, and feeling more attractive. What is not clearly understood is that the “placebo effect” for alcohol is very strong. A wealth of research shows that individuals who believe they are drinking alcohol but actually receive a non-alcoholic drink will report the same positive benefits from drinking. Alcohol expectancy challenge (AEC) programs “challenge” these assumptions about drinking.54-56
Evidence of Effectiveness
Scott-Sheldon et al.57 reviewed the evidence around interventions targeting alcohol use among college students. They found that behavioral interventions during the first year of college that include an AEC were more effective in reducing drinking and harms among college students than those that did not include it. One study compared the drinking behavior of college students assigned to an AEC or a control group.54 Using the Alcohol Expectancy Questionnaire (AEQ) to measure beliefs about outcomes of alcohol use, the researchers showed that the perceived positive effects of alcohol were decreased in the experimental group as compared with controls. Wood et al.56 found that effects lasted three months post-intervention but decayed by six months.
Statmates et al.58 examined the relationship between individuals who were first intoxicated earlier in life and alcohol expectancies. More experienced drinkers were found to have stronger beliefs related to drinking which influenced their drinking behaviors and willingness to change. Madson et al.59 investigated the impact of protective behavioral strategies with an AEC. Among females, but not males, protective behavioral strategies mediated the relationship between positive expectations and drinking quantity.
Another study randomly assigned participants to one of four conditions: BMI, AEC, BMI and AEC combined, and an assessment-only control group.56 While BMI produced significant decreases among all variables, AEC produced significant decreases in measures of total drinks during the past 30 days and frequency of heavy episodic drinking during the past 30 days. AEC conditions showed an increase in intervention effects after three months, but these gains declined completely after six months. This study shows the effectiveness of AEC in the short term but demonstrates the need for it to be accompanied by passive booster sessions.
Tips on Implementation
AEC programs can be implemented in a variety of ways. One prime example is that of a social setting where alcohol and a placebo drink are given to participants in combination with information and education regarding placebo effects.60-62 These types of programs can be implemented in various settings, including residence halls, first-year orientation, and campus organization events.63 Due to the fact that these programs are only effective in the short run, they can be targeted to specific periods of time where alcohol use among the student population might be high (i.e., rush week or spring break).
Strategy: Combine Alcohol and Sexual Assault Prevention
Theory Behind the Strategy
Sexual assault is a serious public health concern, and can be a risk factor for experiencing depression, post-traumatic stress disorder, as well as academic performance problems.64,65 It is estimated that about 20% of women and 6% of men experience some form of sexual assault during their four years in college (although some sources estimate it to be higher among women), with the highest probability of assault during their first two years.66
Reducing excessive drinking as described throughout this Guide should be considered as part of an overall comprehensive sexual assault prevention strategy for college campuses. Alcohol, while never a cause of sexual assault, can be a major contributing factor. Alcohol use by the victim, perpetrator, or both is estimated to be involved in about half of all campus sexual assaults.67-70 Alcohol impairs judgement, dulls senses, slows reflexes, and lowers inhibitions, which has implications not only for victims but perpetrators and bystanders71-74; this makes a sexual assault more likely to happen and less likely to be stopped.
It is important to realize that regardless of whether or not alcohol was involved, victims of sexual assault should be provided the services that they need to manage the aftermath of the trauma experienced. One study found that after a sexual assault in which the victim had consumed alcohol prior to the incident, there was an increased likelihood for alcohol abuse as a means to cope, thus creating a cyclical relationship which puts victims at greater risk for unsafe drinking behaviors and other negative consequences.75
Evidence of Effectiveness
Senn et al.76 conducted an intervention designed to provide college women with strategies to avoid rape at three Canadian universities. The intervention consisted of four three-hour sessions of lectures, games, facilitated discussion, practice activities, and included specific components on excessive drinking.73 The control group received pamphlets about sexual assault, which was the existing practice at the participating universities. After one year, the women who received the intervention experienced a completed rape at about half the rate of the control group (5.2% versus 9.8%), as well as significantly lower rates of attempted rape (3.4% versus 9.3%). Women in the control group who reported being previously victimized had a risk for completed rape that was nearly four times greater than women who had not been previously victimized.
Gilmore et al.77 studied the effectiveness of a web-based program that combined sexual assault prevention and alcohol reduction strategies among college women at high risk for victimization, based on drinking behavior. The combined approach reduced the number of incapacitated rapes, incidence of sexual assault and severity, and frequency of heavy episodic drinking among individuals with a more severe victimization history.
Tips on Implementation
The findings of Senn et al.76 and Gilmore et al.77 are extremely promising, but more research is needed to better understand how alcohol can make a person more susceptible to sexual victimization and how reducing alcohol use should be factored into sexual assault prevention programs on campuses. Certainly, colleges should aim to eliminate stigma related to alcohol-related sexual victimization in order to support victims. Moreover, interventions to reduce excessive drinking should be developed and evaluated as a way to prevent perpetration and improve the capacity of bystanders to effectively intervene. In 2016, Maryland Collaborative staff produced an evidence review summarizing the research on the complex relationship between alcohol and sexual assault on college campuses. This review can be used by educators, administrators, and students as an informational resource as they develop sexual assault prevention programs or activities on campus.[
Educational Approaches
Research studies have consistently demonstrated that while education can increase awareness of alcohol problems and knowledge of alcohol-related risks, it generally does not result in changing behavior. Therefore, universities should not expect that education programs alone will reduce alcohol use or related problems. Educational approaches can assist in increasing awareness of and supporting other types of strategies, such as policy changes or implementation of screening, brief interventions, and referral to treatment.
INVISIBLE - DO NOT DELETE
Strategy: Educate Students about the Dangers of Excessive Drinking
Theory Behind the Strategy
The theory behind educational approaches is that students will be less likely to engage in heavy drinking if they are more aware of the risks involved. Unfortunately, this notion has not been borne out by many years of prevention practice and research. New neurobiological research has shed light on the fact that many college students are developmentally-wired for risk taking and therefore simply educating them about risks will not change their behavior. Some college students have a low level of risk-taking tendencies and might be more susceptible to messages about risk; however, risk-averse students are likely already engaging in heavy drinking.
Evidence of Effectiveness
Alcohol education has very little impact on changing behavior and is not effective as a stand-alone intervention.78 Alcohol education is often used as a control condition in research studies, further highlighting its ineffectiveness as an alcohol reduction strategy. However, it can be incorporated into interventions that include other elements. One study used a mixed-methods approach to evaluate an alcohol education program for use among fraternity members.79 The alcohol education program under study, the Alcohol Skills Training Program, was not found to be effective among this group. Certain components of the program were viewed as useful by the participants, but this did not translate to significant differences in high-risk drinking behavior or negative consequences between test and control groups.
Another study tested the addition of information on alcohol use, decision making, and safety into already existing academic courses instead of making alcohol education its own course, a strategy known as “curriculum infusion.”80 The authors’ analysis found students were engaged in these lesson plans and took the material seriously, but further research is needed to evaluate the effectiveness of this strategy at decreasing alcohol use and related consequences.
Tips on Implementation
Alcohol education can be combined with other intervention strategies that target students who are at risk. For example, a BASICS component for students to explore their alcohol use can be implemented with additional education (either online or in-person programs). More research is needed on the effectiveness of infusing alcohol education into existing course curricula.
Strategy: Utilize Computer-facilitated Educational Approaches
AlcoholEdu
Description
AlcoholEdu for College is a two- to three-hour online alcohol prevention program developed to be made available to an entire population of students, such as an entering first-year class. Educational goals include resetting unrealistic expectations about the effects of alcohol and understanding the link between drinking and academic and personal success.
Evidence of Effectiveness
Five research studies examined alcohol-use outcomes between first-time, incoming college freshman who completed the AlcoholEdu program.48,81-84 Both the intervention and control groups experienced increases in drinking behaviors between high school and the transition to college, but students in the intervention groups had smaller increases in drinking compared with students in the control group.48,83 Significant differences between the two groups of students were found for average number of drinks per week: Hustad et al.48 found that the AlcoholEdu group had a mean increase of 1.5 drinks per week during the past month versus 6.3 drinks among the control group, while Lovecchio, Wyatt, and Dejong83 found a mean increase in total number of drinks during the past two weeks of 4.3 among the AlcoholEdu group versus 8.0 among the control group. A smaller increase was found in heavy drinking episodes per month in the intervention group (increase of 0.6 episodes48 and 19% of students83) than in the control groups (increase of 2.3 episodes48 and 34% of students83). Additionally, the intervention group in Lovecchio’s study reported fewer positive alcohol use expectancies and less acceptance of others’ alcohol use.83
AlcoholEdu also had a small but statistically significant effect on student’s knowledge about alcohol (22.7% score increase for the control condition vs. a 23.4% increase for the intervention condition, p=0.04).83 While one study82 found no significant differences between the two groups for measures of alcohol quantity, further review showed there were baseline differences in parental discussions, alcohol education during high school, and alcohol-related knowledge. Another study had mixed findings on the mediating effects on students’ perceived drinking norms, alcohol expectancies, personal approval of alcohol use, and protective behavioral strategies on the effectiveness of AlcoholEdu.84 Exposure to AlcoholEdu was inversely related to student perceptions of drinking norms, which could have decreased drinking rates and drinking related harms indirectly through changing perceptions, but it did not affect any other psychosocial norms that were targeted.84 Barry et al.81 conducted a qualitative follow-up survey two to four months post-AlcoholEdu intervention. They found an increase in knowledge about alcohol, but there was no change in alcohol-related behavior. Limitations, such as skipping through assessments and video segments without reading or listening, were also noted.
In summary, AlcoholEdu can greatly enhance students’ alcohol knowledge and use of safe drinking practices (including abstaining). However, increased knowledge does not necessarily translate into behavior change. Administrators should be wary of relying solely on this program, as its effects tend to return to baseline by the next semester.85
Tips on Implementation
Administrators who implement AlcoholEdu should consider combining this program with other prevention and intervention programs in order to have a higher magnitude of effect in the long-term. If used, AlcoholEdu should be supplemented with other strategies to screen, identify, and intervene with high-risk drinkers using appropriate and evidence-based methods.
Alcohol 101 Plus
Description
Alcohol 101 Plus is a web-based program that is based off the previous CD-ROM-based version, Alcohol 101. This psychoeducational prevention program consists of an interactive format in a “virtual campus” where the student makes choices about social situations involving alcohol, such as at a party, discusses possible consequences, and considers alternatives. Participants might also visit a “virtual bar” that provides information on their estimated blood alcohol concentration based on number of drinks consumed, weight, and other relevant factors, and can include icons that inform them about alcohol refusal skills, consequences of unsafe sex and underage drinking, comparisons of participant drinking rates with college norm rates, multiple choice games relevant to alcohol, and depictions of real-life campus tragedies involving alcohol misuse.
Evidence of Effectiveness
Four studies compared alcohol-use outcomes among students who drink following completion of the computer-based Alcohol 101 program and other in-person interventions, such as BMI, CBT, and BASICS.86-89 Participants varied between studies, categorized as either violators of alcohol policy who were mandated to complete education,86,88 high-risk drinkers seen at the health clinic,87 or participants from the general student population who reported having at least one drink during the past 30 days.89 Results showed very few advantages of Alcohol 101 interventions over other programs. Carey et al.86 found no effect at a one-month follow-up in mandated female students who completed Alcohol 101, aside from a significant reduction of 0.9 points in the Rutgers Alcohol Problem Index (RAPI; a 23-item screening tool for adolescent problem drinking) score, indicating a small reduction in alcohol-related problems. No reduction was found for males. This reduction was not significantly different from that of individuals in the BMI condition, who also saw a reduction in alcohol quantity, frequency, and BAC. Murphy et al.87 found an average reduction of three drinks per week, but these results were not significantly different from students who received BASICS. However, there was no assessment-only control, so the reduction might not have been an intervention effect.
Another study also found that when compared with BMI, outcomes were similar between groups; both Alcohol 101 and BMI decreased number of drinking days per month by roughly one at the three-month follow-up (1.3 and .5 drinks, respectively), then increased again by approximately 1.5 drinks at 12 months.88 The only demonstrated advantage of Alcohol 101, according to Carey et al.,86 was a decrease in alcohol-related problems, as indicated by the RAPI score. Two of the studies found a general return to baseline drinking after 12 months, despite a brief reduction in drinking at three months.86,88
Tips on Implementation
Little evidence is available that supports the effectiveness of this program to change behavior.
Alcohol-Wise
Description
Alcohol-Wise is an online alcohol abuse prevention course designed for first-year students and other high-risk groups on college campuses. The program takes between one and two hours to complete, and consists of a pre-test of alcohol knowledge, a baseline survey (modeled from eCHUG), educational lessons on alcohol, and a post-test of alcohol knowledge. Alcohol-Wise integrates personalized feedback as students navigate through the program. A baseline follow-up survey is administered about one month after course completion.
Evidence of Effectiveness
Only two studies on Alcohol-Wise were identified. The first presents findings from a randomized controlled trial of 58 undergraduate students assigned to either Alcohol-Wise or a control group.90 After one month, freshman and sophomore students had significant reductions in alcohol use and BAC, but juniors and seniors did not. No significant changes in alcohol expectancies were observed between either the intervention group or control group. The other study examined the short-term effectiveness of Alcohol-Wise among incoming first-year students at two universities.91 Both universities saw a significant increase in alcohol-related knowledge, but effects on drinking behavior were mixed: One university saw a significant reduction in alcohol use and high-risk drinking behaviors such as drinking games and heavy drinking, while the other university did not. Although the authors did not intend to directly compare the two universities, there was substantial variation between the campus types which makes it difficult to conclude whether or not Alcohol-Wise would be effective in other schools.
Settings in Which to Screen, Identify, and Intervene
INVISIBLE: DO NOT DELETE
First-year Orientation
Theory Behind the Strategy
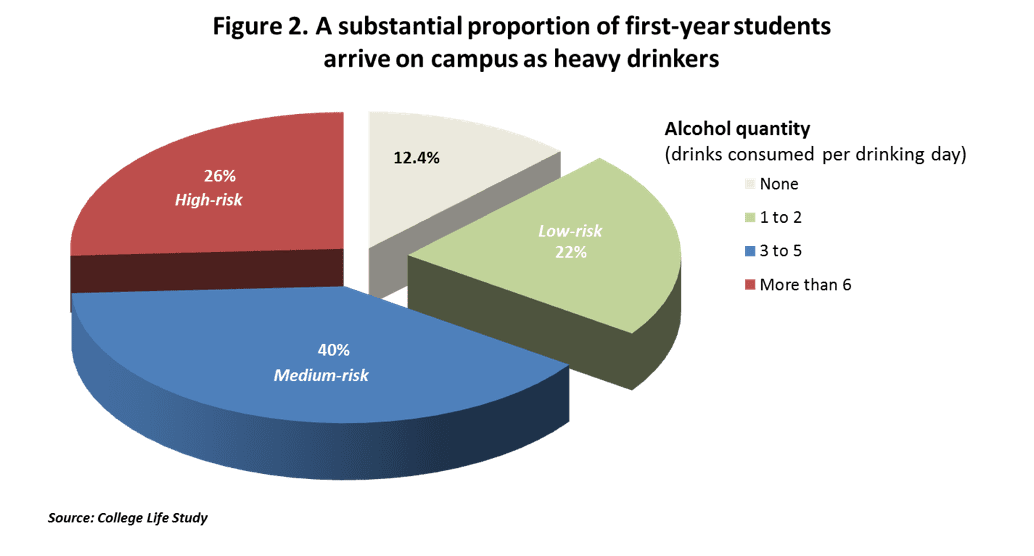
Screening at first-year orientation provides a means of identifying risky drinking practices early through large questionnaire-based screening tools that measure quantity, frequency, and consequences.35 This process can help administrators identify and subsequently refer students for appropriate help. Because some students will enter college with high-risk drinking patterns that began during high school, screening of first-year students is necessary to identify those at highest risk (see Figure 2). Universal screening might be helpful in capturing problems early among incoming students. Screening can occur during orientation or even first-year seminar
classes as a means to identify those who are high risk or have factors that place them at higher risk than others for developing a future problem (e.g., family history, high levels of risk-taking).
Evidence of Effectiveness
One longitudinal study looked at a sample of first-year students and provided confidential questionnaires as part of orientation programs conducted in each
residence hall during the first three weeks of the fall semester with additional follow-up near the end of their junior year (32 months later).92 The survey included variables on quantity and frequency measures as well as problems directly related to alcohol use. The survey also contained questions from the CAGE and the Perceived Benefit of Drinking Scale (PBDS), an index that measures adolescents’ perceived benefits of drinking.
Three categories of students were present among this sample: nondrinkers (11%), low-risk drinkers (51%), and high-risk drinkers (38%). Drinking quantity/frequency during junior year was significantly correlated with quantity/frequency at entry into college (r=0.69, p<0.01). These results support the idea of identifying adolescents at high risk for current or future drinking problems through the screening of first-year students.
Findings from a meta-analysis by Scott-Sheldon et al.57 indicated that individual and group behavioral interventions for first-year college students significantly reduced both alcohol use and problems related to alcohol use with lasting effects up to four years post-intervention. Another study looked at providing a personalized web-based feedback program (eCHUG) for students in a first-year seminar as a means to reduce heavy drinking.93
The sample consisted of low-risk and high-risk drinkers. It was found that high-risk first-year students in the eCHUG group reported a 30% reduction in weekly drinking quantity, 20% reduction in frequency of drinking to intoxication, and 30% reduction in occurrence of alcohol-related problems (as compared with 14%, 16%, and 84% increases, respectively, among the control group). The results of this study revealed that nearly half of the first-year students (41%) reported binge drinking at least once during the past two weeks, and that there was an increase in drinking through the spring for first-year students among the control group.93
Tips on Implementation
Universal screening to identify risky drinking practices early can be done in a variety of ways, and while it might be ambitious and costly (depending on campus size), it can help students access the services they might need.35 Implementing questionnaire screenings in first-year seminar courses or orientation sessions can serve as a basis for identifying potential students who might be at risk for alcohol-related problems. Screening in both the fall and spring semesters should be considered in order to identify these at-risk students.
Primary Health Care
Theory Behind the Strategy
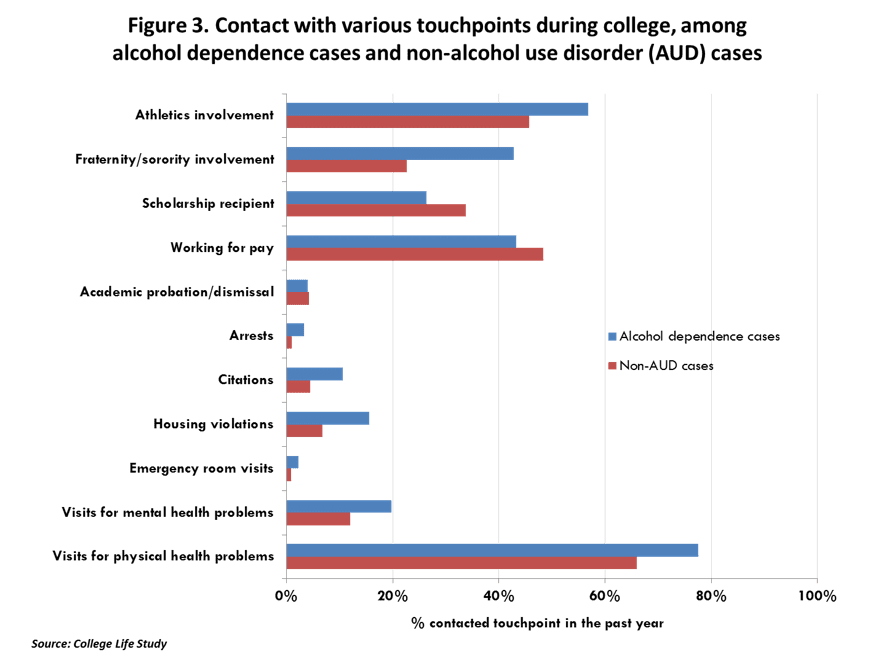
Research has demonstrated that most college students receive services from medical professionals during the course of the school year.94 Because of their frequent contact with students at risk for alcohol-related problems (see Figure 3), it might be worthwhile to train physicians and other allied health care professionals in basic techniques to ask students about their alcohol use patterns as a routine part of care, and intervene when excessive drinking is detected. The U.S. Preventive Services Task Force (USPSTF) recommends that “clinicians screen adults aged 18 years or older for alcohol misuse and provide persons engaged in risky or hazardous drinking with brief behavioral counseling interventions.”95 Integrating questions about alcohol use into routine health care visits can help reduce stigma by placing alcohol use on par with other behaviors that affect health, like eating habits and seat belt use. Alcohol use is associated with a wide range of health consequences, such as decreased immunity, sleep problems, depression, anxiety, and other mental health conditions. Thus, physicians, nurses, and other medical professionals play an important role in intervening with at-risk students if they understand the extent to which alcohol use might be a contributor to the health care complaints of the patient. Physicians and other medical professionals are in a position of professional authority and messages that they convey might be taken more seriously by patients, although this principle might not hold true in the case of young adult college students, who are more likely to be in a developmental stage where questioning authority and feeling invincible are commonplace.
Evidence of Effectiveness
Several studies have demonstrated that physician-delivered advice and brief interventions are associated with reductions in alcohol use among general patient populations. Helmkamp et al.96 demonstrated not only the feasibility of primary care screening, but also found that 96% of participants who screened positively for alcohol dependence after an emergency department visit accepted counseling during their visit. Additionally, participants indicated at follow-up that they found the counseling interventions to be helpful and displayed significantly lower AUDIT scores on all three domains: alcohol intake, alcohol-related harm, and alcohol dependence.
Specific to college students, Amaro et al.97 showed that the BASICS intervention can be delivered within the university health care center with good results; namely, it was associated with reductions in both quantity and frequency of alcohol and other drug use among participants between baseline and six-month follow-up, including a 17% decrease in their weekly heavy episodic drinking during the past month.97 Similarly, in another study of students who screened positively on AUDIT measures and received a basic intervention, drinks per week during the past 30 days were reduced by almost four, peak drinking during the past 30 days was reduced by more than one drink, and number of heavy episodic drinking occasions during the past two weeks was reduced by almost one.98 Schaus et al.99 found that students who screened positive for high-risk drinking after presenting as a new patient at a university health service, those who received a BMI and BASICS had statistically significant reductions over time in drinking behavior outcomes as compared with a control group. More specifically, use fell by an average of 2.2 drinks among the intervention group and 0.7 drinks among the control group at six-month follow-up. These studies provide evidence that interventions delivered by providers within a primary care/health center are effective in reducing negative alcohol behaviors and associated harms, especially among those who are high-risk drinkers.
Another study by Denering and Spear100 analyzed data among 18- to 24-year-olds from a college mental health clinic for routine screening and brief intervention for alcohol and drug use. A slight reduction in the prevalence of binge drinking (90.6% to 88.6% among men and 73.4% to 71.4% among women) was observed, but reductions in the frequency of binge drinking were not significant.100 Although further research is needed to support the use of routine screening in college mental health service settings, the findings from primary care settings could reasonably extend to mental health services.
Tips on Implementation
Because physicians have little time to engage in a meaningful in-depth conversation with their patients, having students complete computerized self-assessments prior to the appointment will save time and perhaps increase the veracity of the patient’s information. The report can then be transmitted to the physician immediately prior to his/her interaction with the patient.
Creating on-campus opportunities to train physicians and other health center personnel can increase the level of comfort with discussing alcohol use, as few medical schools and residency programs provide comprehensive
training on assessment and intervention of substance use. Such trainings should provide research-based information on the connection between alcohol use and several common health complaints of students to help physicians see the value of addressing alcohol use as part of their plan to improve student health.
As mentioned previously, the USPSTF published recommendations in 2013 stipulating that “clinicians screen adults aged 18 years or older for alcohol misuse and provide persons engaged in risky or hazardous drinking with brief behavioral counseling interventions to reduce alcohol misuse,” based on sufficient evidence of the benefits of this approach.95 This web resource might serve as a tool for schools to advocate screening in health centers. Some campuses might house both mental and physical health services under one center; in these environments, it is important for both sides to coordinate efforts to consistently and routinely conduct screening and brief intervention so that students who have or are at risk for alcohol problems can easily be referred to the appropriate treatment or intervention.
Students who Violate Campus Alcohol Policies
Theory Behind the Strategy
Sanctioned students who undergo a mandate for violations of campus alcohol policies and are referred for intervention can cue self-initiated reductions in drinking. Consistent enforcement of policies and sanctions for students who violate alcohol policies can lead to lower heavy drinking rates among students.86 There is general consensus of a “mandate effect”—that is, that no matter what intervention is delivered, there will be reductions in drinking simply because the student has been mandated to receive something. The important implication, therefore, for colleges, is that enforcement of policies—to achieve the goal of identifying students who are violating policies and mandate them to some kind of intervention—is crucial to reduce drinking. Being mandated should be viewed as a “teachable moment” instead of a punishment.
Evidence of Effectiveness
There is evidence to suggest that mandated interventions for students sanctioned for alcohol policies might reduce alcohol use and its consequences.86 Administering BMI with counselor-guided feedback can further reduce alcohol use and consequences. Studies that utilize a no-intervention control group are not possible for ethical reasons. Usually, a two-group or pre-post design is used. Sometimes a “delayed” control is used, consisting of mandated students who are waiting to be seen. Several research studies have evaluated the effectiveness of various types of interventions on mandated students. A 2016 meta-analysis of alcohol interventions among mandated college students found that BASICS and eCHUG were effective in reducing alcohol-related risks in the short-term.46 Terlecki et al.47 found BASICS to be effective in reducing drinking and related problems at one-year follow-up among both heavy-drinking mandated students as well as undergraduates who volunteered to participate. Another study found significant reductions in RAPI scores from baseline to three months and then again from three months to six months in BMI interventions as opposed to usual services for mandated students.101
Additionally, mandated students who received counselor-delivered personal feedback showed a nearly two-drink reduction per week at an eight-month follow-up as opposed to those who received self-guided written feedback who increased their use by almost two drinks per week at follow-up. Furthermore, although those in the counselor-delivered personal feedback group slightly increased their past-two-week heavy episodic drinking (by less than half an episode), this increase was significantly less than those who received self-guided written feedback (who added an entire additional episode per two weeks).37
Tips on Implementation
All mandated students are not the same. Some might have very serious problems and require intensive intervention. Others might present with less severe problems, and perhaps need a lower level of services, but facilitating some sort of intervention for these students is essential to reducing the likelihood that their problem will worsen. Moreover, stories of their experiences will be important for spreading the word among their peers that alcohol violations are taken seriously and result in consequences.
The first step of any mandated program should be a comprehensive assessment of drinking history, current behavior, and problems. Several instruments are available for this purpose. Detailed information about drinking history can flag individuals who are at higher risk than others. For instance, individuals who started drinking prior to age 16 or individuals with a parental history of alcoholism are at greater risk for developing alcohol problems in the future.102,103 Moreover, information should be gathered regarding current problems experienced by the student, such as academic difficulties, health problems, or feelings of depression or lack of motivation. This sort of information related to risk factors and current problems that might be associated with alcohol use can be useful to clinical staff during a brief intervention.
Students Receiving Academic Assistance
Theory Behind the Strategy
There is a strong link between excessive drinking and academic performance problems, including lower grades.18,104 Excessive drinking undermines the learning process in at least two major ways. First, simply the time spent drinking detracts from the time spent on more productive activities, such as studying. Second, students who drink excessively are more likely to skip class and might also experience concentration and memory problems associated with heavy drinking.18
Academic assistance centers typically emphasize strengthening skills that are specific to academics—especially time management and study habits—yet these skills must be applied within the context of whatever barriers to success are presented by the student’s behaviors, choices, and life circumstances. Rather than being a taboo subject that academic counselors avoid, excessive drinking should be taken into account along with other potential barriers to academic functioning such as financial hardship, family problems, and roommate problems.
Students who are receiving academic assistance have taken an important step that demonstrates openness to ameliorating the obstacles to their personal academic success—whether they were referred by someone else or themselves. These students are in a uniquely “teachable moment” with potential to stimulate self-reflection and behavior change in multiple domains of their life. Academic counselors should take advantage of this opportunity to identify students whose drinking habits might be having a negative effect on their grades and refer them as needed for a more comprehensive assessment.
Evidence of Effectiveness
At this time, few schools are implementing screening within academic assistance centers, and therefore little is known about the effectiveness of this strategy. However, to the extent that it results in more high-risk students being referred for screening and brief intervention, we are convinced that it has great potential for reducing excessive alcohol use, as well as for enhancing academic outcomes.
Tips on Implementation
Staff working in academic assistance centers could be trained to administer a simple screening instrument to students at the time of intake. Similar to health care service settings, where staff time is valuable, it might be less costly to have students complete computerized self-assessments prior to the appointment. Transmitting the report to the staff member immediately prior to the appointment might alleviate their discomfort in having to directly ask about the student’s alcohol use.
Creating on-campus opportunities to train academic assistance personnel about how to discuss alcohol use can increase their level of comfort with this sensitive topic. Training should include research-based information on the connection between alcohol use and academic performance, which will help academic counselors see the importance of addressing alcohol use as part of their plan to help the student improve his/her study habits and overall academic performance.
Athletic Programs
Theory Behind the Strategy
Athletes are at high risk for problem alcohol use and related consequences.105-108 Studies have shown that athletes consume more alcohol and experience higher rates of alcohol-related consequences as compared with their non-athlete colleagues.109 Apart from the risk for unintentional injury, alcohol use can negatively impact performance and recovery in athletes.110,111 Screening athletes in college/university athletic programs is an important means of identifying students since they are a target group for heavy drinking. Screening can take place during student-athlete orientation prior to the start of the first year with follow-up programs throughout the year. Identifying these students in this group early on can help move students to appropriate services and treatment. Coaches, team leaders, and athletic trainers are highly influential in the lives of athletes, and therefore can be important partners in programs targeting student-athletes.
Evidence of Effectiveness
A study by Doumas et al.112 compared heavy drinking and alcohol-related consequences among first-year student-athletes and non-athletes, and found that first-year athletes reported higher levels of drinking, drunkenness, and academic, interpersonal, physical, and dangerous consequences than their counterparts. Student-athletes were asked about quantity of drinking on the weekend and frequency of drunkenness, as well as alcohol-related consequences using tools like the Daily Drinking Questionnaire (DDQ) and the Young Adult Alcohol Problems Screening Test (YAAPST). It was found that athletes reported heavier drinking as compared with non-athletes in the fall that intensified in the spring term.
For student-athletes, it is important to consider the timing of strategies, as their athlete orientation programs generally occur at the beginning of each term. College administrators might want to consider providing screening and intervention programs throughout the academic year in order to provide continuous monitoring of alcohol problems among students. It is also important to consider who specifically can and will provide an intervention for student-athletes, such as coaches or athletic trainers. A recent review on alcohol-related unintentional injury among college athletes states that athletic trainers “have the capability and responsibility to play active roles as integral members of the health care team,” but lack the confidence or self-efficacy to do this.113 Intervention involving athletic trainers will require further research into how to best develop and adapt existing screening and brief interventions based on the trainer’s experience and confidence in addressing alcohol problems with student-athletes.113 Additionally, norms modeled by coaches and teammates might discourage or promote drinking; thus, taking action such as setting team policies around alcohol use could be beneficial.114
Research supports the idea that BMIs are effective in reducing heavy drinking among college students, particularly first-year student-athletes. Another study by Doumas et al.115 examined an intervention program for student-athletes as part of first-year seminar curriculum. The program implemented, eCHUG, is designed to reduce high-risk drinking through feedback and normative data around drinking and associated risks. High-risk students in the study’s intervention group reported reductions in weekly drinking (46%), frequency of drinking to intoxication (46%), and peak alcohol use (32%), compared with increases among the comparison group (21%, 6%, and 11% respectively). Since athletic staff and university personnel need to recognize that heavy drinking can progress through the year, implementing programs periodically throughout the year might be beneficial.
Tips on Implementation
Providing screening programs for first-year student-athletes is an important tool to identify students who might be at high risk for coming in with or developing drinking problems. University personnel and athletic staff can work to incorporate web-based personalized normative feedback programs or screening questionnaires during athletic orientations or first-year seminar courses to target all incoming athletes. This can be done during the fall and spring semesters of the first year in order to reduce heavy drinking that might occur during this time. Athletic programs might also want to consider frequent screenings throughout the year as heavy drinking can occur as the year progresses.
Fraternities and Sororities
See section on Risk Managers in the Greek System in Provide Supportive Coaching to Key Individuals on Campus
Provide Supportive Coaching to Key Individuals on Campus
INVISIBLE - DO NOT DELETE
Resident Advisors
Goals
- To increase resident advisors’ (RAs’) knowledge of the nature and extent of the problem
- To increase their capacity to identify high-risk students and make appropriate referrals
- To increase their ability to manage alcohol-related incidents
Theory Behind the Strategy
The primary responsibilities of RAs include: 1) recognizing and responding to students who might need help; and 2) enforcing campus alcohol policies. Boosting the quality of the initial and ongoing training of RAs will empower these individuals to take proactive action and identify students with possible alcohol problems that are in need of more intensive intervention. Because of the high proportion of students living in residence halls on some campuses, training RAs has the potential to reach a large number of students. Moreover, training RAs can facilitate a shared understanding of the problems and risks associated with alcohol use and help spread a common message about the seriousness of violating campus alcohol policies and underage drinking laws.
Evidence of Effectiveness
While few formal research studies have directly evaluated the effectiveness of training RAs, increasing awareness about the seriousness of the problem, and empowering them to identify high-risk students and manage alcohol-related incidents more efficiently and effectively is good common sense. A national study found that 31% of students meet psychiatric criteria for alcohol abuse and 6% for alcohol dependence; with 43% of participants living in university housing such as residence halls and fraternity/sorority housing.116 Because research has demonstrated that it is possible to train individuals to screen and identify high-risk drinkers, RAs should receive ongoing training regarding warning signs and symptoms of alcohol problems. NIAAA recommends keeping RAs involved in planning and implementing campus alcohol policies and programs.117
Tips for Implementation
Initial trainings for RAs could include topics such as: 1) tips on how to have discussions with student residents about the risks of underage and excessive drinking; 2) campus alcohol policies and sanctions; 3) identifying at-risk students; and 4) managing alcohol-related incidents. Alcohol-related topics should be incorporated into initial RA training sessions, and followed up by ongoing—at least annual—training events for RAs that can keep them abreast of necessary skills and re-educate them about the procedures to manage students who might exhibit problems related to alcohol. Such events could include opportunities to share experiences.
Faculty
Goals
- To increase faculty knowledge of the nature and extent of the problem
- To increase their capacity to identify high-risk students and make appropriate referrals
Theory Behind the Strategy
Faculty are in a position to act on obvious signs of problems, such as coming to class intoxicated. By virtue of the fact that faculty, especially those who teach small- to mid-size classes, are in regular contact with students, they are likely to notice subtler but significant changes in behavior that might signal an alcohol problem. Namely, faculty might be aware of particular students who are chronically absent or academically struggling—possible warning signs of excessive drinking. In these cases, if trained, they would be in a position to make a referral to that student to seek appropriate help.
Evidence of Effectiveness
The evidence linking excessive drinking and other drug use with decreases in academic performance (e.g., GPA) or engagement (e.g., skipping class) is extensive.18,19 While few studies have addressed faculty training for alcohol problems, many colleges and universities have implemented “gatekeeper training” as a means to identify students at risk for suicidal behaviors. Gatekeeper training has several key components: 1) detecting students at-risk, 2) implementing crisis intervention, and 3) referring students to appropriate treatment resources.118 A similar approach can help faculty identify students who might be at high risk for developing alcohol problems, especially if students are not self-identifying.
Syracuse University’s (SU) gatekeeper training model, Campus Connect, focuses on information sharing and experiential tools to increase knowledge, awareness, and skills concerning college student suicide.119 Not only are gatekeepers able to more effectively respond to needs and provide resources, but this type of training also enables gatekeepers to respond caringly and efficiently to students with a wide range of crises. Those who are trained and act as gatekeepers are typically administrators and staff, including those involved with Student Affairs, Residence Life, Health Services, Faculty/Academic Counseling, Peer Education, etc. An evaluation of the Campus Connect program at SU demonstrated a significant increase in gatekeeper knowledge, skills, and comfort in responding to students in crisis.120
Instituting Friday morning classes as a means to deter drinking during the week is a National College Health Improvement Project (NCHIP) strategy to address high-risk drinking. College students with later classes are at a greater risk for increased alcohol use, which in turn can have a strong effect on academic performance.121 In a study by Wood et al.,122 it was found that Friday class schedule was an effective predictor of heavy Thursday night drinking, where students with no Friday classes and students with classes beginning at 12pm or later drank approximately twice as much on Thursdays as students with early Friday classes. This effect was amplified among males and among members of and participators in Greek life. Similarly, Hoeppner et al.123 examined daily drinking patterns of first-year college students. Thursday drinkers were less engaged academically and were more likely to participate in risky drinking behaviors.
One campus that has implemented this strategy and has been a model in reducing excessive drinking on and off campus is Frostburg State University. Knowing that students sometimes begin their weekends on Thursday nights (nationally known as “Thirsty Thursdays”), the President’s Alcohol Task Force encouraged educators to offer more Friday classes where assignments are due and quizzes are given. According to Frostburg’s College of Business, implementation of this strategy has led to students reporting reduced drinking.124
Tips for Implementation
Multiple opportunities exist for providing support to faculty that might not require much additional logistical coordination. For example, there are regularly scheduled departmental meetings for faculty, to which guest speakers could be invited. A key person from the Faculty Senate can serve as a member of the Campus Coalition and disseminate information related to how to address alcohol problems among students and campus alcohol policies. Importantly, the idea is not to turn faculty into therapists or counselors, but rather enable them to facilitate student access to appropriate resources to get help. Faculty should feel empowered to provide such information, and regular exposure to information and training opportunities can help them achieve that goal. Importantly, training should be ongoing rather than a one-time event, and can be facilitated through the use of webinars and other online training resources.
Risk Managers in the Greek System
CONTENT
Students
Goals
- To increase students’ knowledge of the nature and extent of the problem
- To increase their capacity to recognize signs of alcohol problems among their peers
- To empower them to facilitate appropriate referrals for further assessment
- To increase the likelihood that they will seek proper medical attention for themselves and their peers in emergency situations
Theory Behind the Strategy
Empowering students to recognize high-risk drinking among their peers might help them to persuade their peers to be screened more formally for an alcohol problem. Known as the “bystander effect,” this phrase is used to describe situations in which those who witness a person in need of help choose not to provide the help that is needed. Preparing students to recognize signs of alcohol problems and to take positive action will result in increased knowledge and awareness to identify those who need help. For situations where risk is immediate and acute, students should be trained to assess signs or symptoms of alcohol poisoning and what actions can be taken (i.e., call 911 or the health center on campus). Additionally, as they observe their peers over the long term, students can be trained to recognize signs of alcohol dependence and how to facilitate referral to appropriate care as a way of providing support to their peers in a non-confrontational, non-judgmental manner.
Evidence of Effectiveness
One study revealed that a majority of students report showing helping behaviors and concern for their peers, especially around alcohol poisoning symptoms.93 In this study, while a majority of students (57.8%) had identified and helped another individual in need, there are still barriers students face when choosing whether or not to help another. Of those students who reported to not have helped another student in an alcohol related emergency (n=43), most reported to not believe the student in need was at risk or needed help.131 This study demonstrates the importance of providing alcohol education for students through a variety of sources, including online resources that contain easily accessible information on symptoms of alcohol poisoning with instructions on when and how to help. A later study confirmed this theory, finding that 65% of students reported that they would help in a hypothetical alcohol-related emergency after seeing an online video detailing the symptoms of alcohol overdose and how to help a student in need. This was an improvement over the 57% of those in the control comparison group who reported that they would help.132 However, another study found that students struggled to correctly identify signs of alcohol poisoning.133
Another study measured student blood or breath alcohol levels after referral for emergency medical evaluation, following implementation of a campus policy in which students exhibiting any signs of intoxication were required to be taken to emergency departments.134 Admissions to the emergency department increased, which is expected, but the mean alcohol level did not change and students frequently drank to toxicity; in other words, the policy appeared to funnel more students who were indeed at risk for alcohol poisoning into the emergency department, but who might not have come otherwise. These findings are similar to that of a previous study conducted in 2012 in which admissions increased but average blood alcohol content did not following the implementation of a collegiate-based medical emergency transport service.135
Tips for Implementation
Training students to identify alcohol problems among their peers can be a strategy that not only protects their peers, but helps students recognize any associated alcohol problems they themselves might be facing. Implementing this type of training around warning signs, signs and symptoms of alcohol poisoning, resources to help, etc. during orientation and first-year seminar courses can be a significant way to target students as they matriculate into college.
Medical Amnesty
Theory Behind the Policy
Medical Amnesty is a policy that schools can use to encourage students to recognize warning signs of alcohol poisoning and to seek appropriate medical assistance in cases of an alcohol-related emergency. Oftentimes, students are afraid to assist a peer or receive individual help in alcohol-related situations because of sanctions and disciplinary processes that might follow. However, amnesty policies might contribute to a higher level of helping behavior as students bypass disciplinary actions to get interventional help.
In many cases, institutions use the terms “Medical Amnesty” and “Good Samaritan” policies interchangeably. However, some schools make the distinction between the two policies. In these cases, Medical Amnesty is a policy that protects students from campus judicial sanctions when they consume alcohol to a dangerous level and might need to receive medical assistance.136 Medical Amnesty policies might also be passed at the state level, providing the same protection. On the other hand, Good Samaritan policies provide students amnesty from campus judicial sanctions in alcohol-related situations where a student might call for help for a peer who has over-consumed alcohol.132 Both the helper and the drinker are provided amnesty from consequences around policy violations in these cases.132 Typically, amnesty is granted if the individual(s) comply with completing an intervention or alcohol education program.
As such, Medical Amnesty should not be viewed as a way to reduce the overall level of excessive drinking on campus, but rather a possible way to reduce the most severe physical harms associated with alcohol overdose. If implemented correctly, the goal is to save lives by placing an individual who has overdosed in the immediate care of a health professional, as has been shown in case studies of the policy.137 Additionally, Medical Amnesty can also provide an opportunity for follow-up intervention after the acute crisis has subsided.
Evidence of Effectiveness
The creation of the Medical Amnesty policy at Cornell University was in accordance with the protocol of dealing with alcohol-related emergencies.137 A marketing campaign helped inform students of this policy through the display of posters in residence halls, academic buildings, fraternities/sororities, ads in newspapers, table tents in dining halls, etc. These tactics helped to raise knowledge and awareness among students that the policy even existed.
After implementation of the Medical Amnesty policy at Cornell University, the percentage of students who actually called for help increased. The number of students who reported they did not call for help out of fear of getting in trouble decreased by 61%, and alcohol-related Emergency Medical Services calls increased by 22% in the two years following the Medical Amnesty policy’s implementation. The percentage of students who received educational or counseling follow-ups after a medical transport more than doubled from 22% to 52%.137
Another study examined the impact of a Medical Amnesty policy and an online alcohol poisoning video on student intentions to seek help during incidents of alcohol poisoning.132 Students who received both an alcohol-poisoning educational video and information about the school’s Medical Amnesty policy were 78% more likely to help in a hypothetical situation, as opposed to 74% who only saw the Medical Amnesty policy, 65% who only watched the video, and 58% who saw neither. The researchers found that particular groups of people, including women, abstainers, and students who had not been exposed to an alcohol poisoning situation during the past, would be more likely to call for help. The study suggested looking for strategies to affirm the tendency in less experienced drinkers while also targeting heavier drinkers with educational strategies as an attempt to increase this behavior.
Tips for Implementation
Several conditions are necessary for effective implementation of a Medical Amnesty policy. First, it is crucial to successfully market the policy to raise awareness about the existence of the policy. Administrators should frame these policies as a means to educate students and create conditions that should be promoted both on and off campus rather than as punishments. Students should be made aware that while they will be treated fairly for doing the right thing or helping their peers, they will also be held accountable for their behavior through mandated intervention and follow-up.
Additionally, education can be provided to students about the signs of overdose as well as who and how to call for help in alcohol-related emergencies. Education can be provided through a variety of methods, such as online videos about recognizing signs and symptoms of overdose, email reminders about helping behaviors, and discussions with RAs. Schools should mandate follow-up assessments and counseling in lieu of punishment as a means of promoting student success.
Collegiate Recovery Programs
Theory Behind the Strategy
Students who arrive on campus with a history of substance abuse issues face unique challenges: balancing recovery activities with coursework, forming a social life while abstaining from drinking, and living in dormitories, environments often perceived as harmful to recovery.138,139 An on-campus recovery program enables these individuals to obtain social support and a sense of security from a community of peers who are facing similar challenges.138 Additionally, on-campus students in recovery can serve as role models for other students struggling with substance abuse issues.140 The Association of Recovery in Higher Education (ARHE) is a network of U.S. colleges and universities that have embraced a shared mission of supporting students in recovery.141,142 Their website provides several resources for campuses interested in starting collegiate recovery programs.
Evidence of Effectiveness
Anecdotal data suggest that among students with a history of substance abuse, participation in collegiate recovery programs is associated with higher academic achievement and better retention rates. Moreover, four years of data from the Center for Collegiate Recovery Communities (CRC) at Texas Tech University suggest its members have higher graduation rates and GPAs than the general student population, as well as low relapse rates.143-145
Tips for Implementation
College-based recovery programs do more than simply refer students to off-campus resources such as Alcoholics Anonymous or Narcotics Anonymous meetings. In successful collegiate recovery programs, participants receive their key support from the community itself, with individual students both giving and receiving assistance.138,146 Furthermore, the most successful programs also integrate professional services (counseling) with peer support and help students address academic issues.146 According to Laudet et al.,145,147 typical components of collegiate recovery programs include 12-step programs based on campus, substance-free housing, and professional counseling by addiction treatment specialists, to name a few. The Study of Addiction and Recovery (CSAR) at Texas Tech University has developed a curriculum designed to guide other colleges in the process of developing recovery support communities; a full copy can be obtained directly from the CSAR.146,148
Another option is to offer recovery housing, which goes beyond “substance-free housing.” For example, in 1998, Rutgers University implemented the Alcohol and Other Drug Assistance Program (ADAP). The program offers recovery housing where residents have easy access to recovery counseling, general psychological counseling, medical services, on-campus 12-step meetings, an advisor for academic and career support, and organized group activities such as plays, hikes, and bike trips.149 Another challenge to implementing a comprehensive collegiate recovery program is cost to the student; one study identified financial concerns as a major source of stress for students in recovery.139 Texas Tech University began providing merit-based scholarships to students to their program.150
In 2016 Maryland Collaborative staff produced a brief report that describes what collegiate recovery programs are, their benefits, and highlights what some colleges are doing to support students who are in recovery from substance use disorders. This resource can be used by students, staff, and faculty to help raise awareness about the need for collegiate recovery programs and advocate for their implementation on campus.
Medical Amnesty
Theory Behind the Policy
Medical Amnesty is a policy that schools can use to encourage students to recognize warning signs of alcohol poisoning and to seek appropriate medical assistance in cases of an alcohol-related emergency. Oftentimes, students are afraid to assist a peer or receive individual help in alcohol-related situations because of sanctions and disciplinary processes that might follow. However, amnesty policies might contribute to a higher level of helping behavior as students bypass disciplinary actions to get interventional help.
In many cases, institutions use the terms “Medical Amnesty” and “Good Samaritan” policies interchangeably. However, some schools make the distinction between the two policies. In these cases, Medical Amnesty is a policy that protects students from campus judicial sanctions when they consume alcohol to a dangerous level and might need to receive medical assistance.136 Medical Amnesty policies might also be passed at the state level, providing the same protection. On the other hand, Good Samaritan policies provide students amnesty from campus judicial sanctions in alcohol-related situations where a student might call for help for a peer who has over-consumed alcohol.132 Both the helper and the drinker are provided amnesty from consequences around policy violations in these cases.132 Typically, amnesty is granted if the individual(s) comply with completing an intervention or alcohol education program.
As such, Medical Amnesty should not be viewed as a way to reduce the overall level of excessive drinking on campus, but rather a possible way to reduce the most severe physical harms associated with alcohol overdose. If implemented correctly, the goal is to save lives by placing an individual who has overdosed in the immediate care of a health professional, as has been shown in case studies of the policy.137 Additionally, Medical Amnesty can also provide an opportunity for follow-up intervention after the acute crisis has subsided.
Evidence of Effectiveness
The creation of the Medical Amnesty policy at Cornell University was in accordance with the protocol of dealing with alcohol-related emergencies.137 A marketing campaign helped inform students of this policy through the display of posters in residence halls, academic buildings, fraternities/sororities, ads in newspapers, table tents in dining halls, etc. These tactics helped to raise knowledge and awareness among students that the policy even existed.
After implementation of the Medical Amnesty policy at Cornell University, the percentage of students who actually called for help increased. The number of students who reported they did not call for help out of fear of getting in trouble decreased by 61%, and alcohol-related Emergency Medical Services calls increased by 22% in the two years following the Medical Amnesty policy’s implementation. The percentage of students who received educational or counseling follow-ups after a medical transport more than doubled from 22% to 52%.137
Another study examined the impact of a Medical Amnesty policy and an online alcohol poisoning video on student intentions to seek help during incidents of alcohol poisoning.132 Students who received both an alcohol-poisoning educational video and information about the school’s Medical Amnesty policy were 78% more likely to help in a hypothetical situation, as opposed to 74% who only saw the Medical Amnesty policy, 65% who only watched the video, and 58% who saw neither. The researchers found that particular groups of people, including women, abstainers, and students who had not been exposed to an alcohol poisoning situation during the past, would be more likely to call for help. The study suggested looking for strategies to affirm the tendency in less experienced drinkers while also targeting heavier drinkers with educational strategies as an attempt to increase this behavior.
Tips for Implementation
Several conditions are necessary for effective implementation of a Medical Amnesty policy. First, it is crucial to successfully market the policy to raise awareness about the existence of the policy. Administrators should frame these policies as a means to educate students and create conditions that should be promoted both on and off campus rather than as punishments. Students should be made aware that while they will be treated fairly for doing the right thing or helping their peers, they will also be held accountable for their behavior through mandated intervention and follow-up.
Additionally, education can be provided to students about the signs of overdose as well as who and how to call for help in alcohol-related emergencies. Education can be provided through a variety of methods, such as online videos about recognizing signs and symptoms of overdose, email reminders about helping behaviors, and discussions with RAs. Schools should mandate follow-up assessments and counseling in lieu of punishment as a means of promoting student success.
Collegiate Recovery Programs
Theory Behind the Strategy
Students who arrive on campus with a history of substance abuse issues face unique challenges: balancing recovery activities with coursework, forming a social life while abstaining from drinking, and living in dormitories, environments often perceived as harmful to recovery.138,139 An on-campus recovery program enables these individuals to obtain social support and a sense of security from a community of peers who are facing similar challenges.138 Additionally, on-campus students in recovery can serve as role models for other students struggling with substance abuse issues.140 The Association of Recovery in Higher Education (ARHE) is a network of U.S. colleges and universities that have embraced a shared mission of supporting students in recovery.141,142 Their website provides several resources for campuses interested in starting collegiate recovery programs.
Evidence of Effectiveness
Anecdotal data suggest that among students with a history of substance abuse, participation in collegiate recovery programs is associated with higher academic achievement and better retention rates. Moreover, four years of data from the Center for Collegiate Recovery Communities (CRC) at Texas Tech University suggest its members have higher graduation rates and GPAs than the general student population, as well as low relapse rates.143-145
Tips for Implementation
College-based recovery programs do more than simply refer students to off-campus resources such as Alcoholics Anonymous or Narcotics Anonymous meetings. In successful collegiate recovery programs, participants receive their key support from the community itself, with individual students both giving and receiving assistance.138,146 Furthermore, the most successful programs also integrate professional services (counseling) with peer support and help students address academic issues.146 According to Laudet et al.,145,147 typical components of collegiate recovery programs include 12-step programs based on campus, substance-free housing, and professional counseling by addiction treatment specialists, to name a few. The Study of Addiction and Recovery (CSAR) at Texas Tech University has developed a curriculum designed to guide other colleges in the process of developing recovery support communities; a full copy can be obtained directly from the CSAR.146,148
Another option is to offer recovery housing, which goes beyond “substance-free housing.” For example, in 1998, Rutgers University implemented the Alcohol and Other Drug Assistance Program (ADAP). The program offers recovery housing where residents have easy access to recovery counseling, general psychological counseling, medical services, on-campus 12-step meetings, an advisor for academic and career support, and organized group activities such as plays, hikes, and bike trips.149 Another challenge to implementing a comprehensive collegiate recovery program is cost to the student; one study identified financial concerns as a major source of stress for students in recovery.139 Texas Tech University began providing merit-based scholarships to students to their program.150
In 2016 Maryland Collaborative staff produced a brief report that describes what collegiate recovery programs are, their benefits, and highlights what some colleges are doing to support students who are in recovery from substance use disorders. This resource can be used by students, staff, and faculty to help raise awareness about the need for collegiate recovery programs and advocate for their implementation on campus.
Connecting with Parents as Partners
INVISIBLE - DO NOT DELETE
Theory Behind the Strategy
Theory Behind the Strategy
Despite the strong influence that peers have on student drinking—both before and during college—parents are also a very important source of influence. Parents’ influence begins long before college entry and occurs through three main mechanisms. First, parents convey messages (both implicitly and explicitly) to their children about their expectations concerning alcohol use. When parents convey consistent disapproval of underage drinking, adolescents tend to have less alcohol involvement than their peers whose parents convey more accepting or equivocal attitudes.151 Second, students are influenced by the drinking behaviors their parents model, whether those drinking patterns are responsible or irresponsible, but this might not always have a “consistent impact.”152 Third, during high school, parents exert their influence by setting rules and monitoring the whereabouts, activities, and peer group of their adolescent child, which is a key factor in deterring heavier drinking.151,153
As students begin college, two important changes occur—namely, their parents monitor their activities less, and they experience increasing peer influences—all of which increases the opportunities for substance use.154,155 Moving out of a parent’s home and into the residence halls or off-campus housing can also increase the opportunities for heavy drinking.155
Even though parents might no longer be physically present on a day-to-day basis, their influence persists indirectly through the habits, attitudes, and values that they helped to engender throughout childhood and adolescence. Although the frequency and manner of parent-child interactions will change during college, they continue to have the potential to reinforce the messages and values that were instilled earlier.
Moreover, by maintaining open lines of communication, parents can monitor their college-attending child for signs that their alcohol use might be escalating into a serious problem. For example, academic struggles, emotional problems, and conflicts with roommates or friends could be symptomatic of excessive drinking.
We will describe four strategies for involving parents during three crucial time periods in students’ college experience: pre-matriculation, the first year, and succeeding years.
Strategy: Provide Pre-matriculation Educational Materials to Parents
Theory Behind the Strategy
High school can be an opportune time for parents to have conversations with their children about the consequences of excessive drinking. For instance, when students get their college acceptance letters (generally while they are still in high school), administrators could include a brochure to parents urging them to talk to their students about alcohol. The Maryland Collaborative staff developed the parent-focused website College Parents Matter in 2015, which contains general tips on communication and specific conversation starters for parents to speak with their college-age child about different high-risk drinking situations.
Evidence of Effectiveness
Parent-based interventions during the transition to college have been repeatedly shown to be effective in reducing students’ alcohol use during college,156,157 for example, cutting drinking by almost half (8.1 drinks vs. 4.4 drinks per weekend).157 Several studies have also looked at the effectiveness of parental interventions to reduce high-risk college drinking. A study by Turrisi et al.158 examined high-risk college students who were randomized into one of four conditions: a parent intervention, a BASICS intervention (for the student), a combined condition (parent intervention plus BASICS), or an assessment-only control group. The parent intervention, which took place during the summer prior to college matriculation, included a 35-page handbook that discussed student drinking, effective strategies for communicating with teenagers, and how alcohol affects the body. The study found that participants in the combined condition and the BASICS-only condition reported approximately one fewer drink per week, one fewer drink per weekend, and fewer alcohol-related consequences than participants in the control group or the parent-only intervention. Participants in the combined condition reported fewer alcohol-related consequences than the BASICS-only condition. This study suggests that parental intervention delivered before college can enhance the efficacy of BASICS.
Another study by Turrisi et al.159 examined college freshman attitudes toward drinking and alternatives to drinking on the weekend. Parents in the intervention group were provided with the 35-page handbook the summer before college matriculation with information about parent-teen communication and college drinking. Eighty-seven percent of the parents returned the handbook with written comments showing that parents actually read the materials. The intervention and control groups were significantly different when it came to demonstrating the efficacy of the parent intervention. For example, college students whose parents were in the intervention group had more positive attitudes toward alternative activities (i.e., going to a sporting event or a coffee shop) than did individuals in the comparison group. Those in the comparison group believed that alcohol had greater perceived benefits (i.e., alcohol enhances social behavior and alcohol creates positive transitions) as compared with the intervention group. The results from this study suggest that a parent-based intervention can work to change teens’ attitudes and beliefs about drinking and non-drinking alternatives.
A follow-up study by Cleveland et al.160 had mixed results on the effectiveness of a parent-based intervention administered before entering college, and the authors recommend further research.
Strategy: Keep Parents Involved during the First Year of College
Theory Behind the Strategy
Though going away to college does create some distance, parents can still serve as a protective influence for their college-attending child. Keeping parents involved in their child’s life, especially during the first year of college, can encourage protective discourse. Administrators should update parents with facts about alcohol and its consequences, specific alcohol-related campus policies, alcohol-related events in the news, and ways to discuss these matters with their child. The first few weeks that their child is on campus is a critical time for parents to stay actively involved. For example, parents might want to know the school’s policies around alcohol, make regular contact with their child, and inquire about their child’s residence and who they live with. Parents should also discuss the risks associated with underage drinking, such as sexual aggression or victimization, violence, and academic failure.”161
Evidence of Effectiveness
Parents who receive an invitation to an online alcohol-education program (MyStudentBody, for example) are more likely to discuss responsible alcohol use with their college-attending child. Additionally, first-year students whose parents received alcohol education reported safer drinking practices.162
Strategy: Maintain Involvement of Parents
Theory Behind the Strategy
Communication and setting boundaries are important in both preparing a child for college and staying involved on an ongoing basis. Parents should be encouraged to keep up discussions with their child about the risks associated with excessive drinking, and clearly articulate their expectations about avoiding alcohol if they are underage or drinking responsibly if they are of legal age. According to a study of a web-based parent intervention, parents and teens appear to be confident in discussing alcohol, drug, and other related issues.162 A parent-focused website, College Parents Matter, was developed by the Maryland Collaborative in 2015 and provides tips and scripts to help parents communicate effectively with their college-aged child about high-risk drinking situations.
Parents’ weekend is an ideal time for colleges to involve parents in discussions about alcohol-related issues. For example, colleges can deliver informational presentations and distribute printed material describing what campus resources are available for students who might have a drinking problem. These interventions should be designed to stimulate conversations about alcohol between parents and students, and to encourage ongoing parent-child communication overall.
Evidence of Effectiveness
Regular parent-child communication during college has been shown to be a protective factor against excessive drinking. On days in which first-year students spoke with their parents for at least 30 minutes they consumed 20% fewer drinks and were 32% less likely to engage in heavy episodic drinking compared with days that they did not communicate with their parent.163 Doumas et al.164 evaluated a parent-based intervention among first-year students whose parents received either a handbook for parents, a handbook plus a series of three booster brochures sent to the parents throughout one semester, and a control group. They found no significant differences in student drinking behavior between the handbook-only and control group, but the handbook plus booster brochure group reported significantly less drinking than the handbook-only and control groups. These findings suggest that additional materials that remind or reiterate the message to parents throughout the academic semester might enhance effectiveness of a parent-based intervention.
Strategy: Parental Notification of Alcohol-related Incidents
Theory Behind the Strategy
Following a 1998 amendment to the Family Educational Rights and Privacy Act (FERPA), schools are allowed to contact parents when their student under 21 is found guilty of an alcohol or drug violation.165 Notifying parents about possible drug or alcohol problems following an early violation might help prevent larger, more dangerous consequences in the future. Parental notification policies are intended to increase parent involvement in their students’ decisions about alcohol use.165
More specifically, parental notification policies are helpful in motivating students to deter alcohol abuse and risky behaviors in order to avoid parent communication with their university regarding substance use. The policies help to increase student safety for those students who have already committed violations/broken school policies through parental involvement in their child’s health-related problems.165
Evidence of Effectiveness
Several studies have examined the effect of parental notification on alcohol problems on college campuses. An examination of 349 higher education institutions by Lowery et al.166 found that those with parental notification policies had “slightly (44.4%) or significantly (11.3%) reduced the overall number of alcohol-related violations.” The authors reported that 74% of institutions with parental notification policies had slightly (48%) or significantly (26%) lowered the rate of repeat on-campus violations.
The effectiveness of parental notification policies is both a function of how they might serve as a deterrent as well as the types of actions that are taken by parents who are notified. A majority of parents (96%) discussed the arrest or citation as well as alcohol/substance use with their child. Many parents (67%) also found that a positive behavior change resulted from the notification policy, and a very small percentage (2%) reported negative behaviors. Almost half of parents reported giving their child a consequence once they were notified (44%). Some of the consequences that parents cited included paying a fine, losing car access, or losing parental monetary support.165,166
A 2000 survey167 of 189 public and private schools conducted by Bowling Green State University and the Association for Student Judicial Affairs Model Policy Committee found that 59% of schools had either a practiced or written parental notification policy. An additional 25% of schools were considering adopting a notification policy, and only 15% said that they did not plan to implement any policy. The study also found wide support for notification policies among parents, of whom 79% were either very or somewhat supportive.